Unpacking the 2.5 billion without access

Most of our national WASH statistics mask groups of people belonging to the poorest and most marginalised. These groups often constitute the unserved. When we say that over 2.5 billion people in the world lack access to safe sanitation and hygiene, do we actually know which of this number represents the poorest in society, or how many of them live in remote or inaccessible areas?
“People like me are considered a burden in society. As I cannot walk and I need assistance for everything – I am like a prisoner. We are a forgotten lot – invisible. I am usually not invited to any events and meetings. They just presume I cannot come physically. For me every party, community event, or festival are times to mourn. I love going to these places, but my family never takes me.” (Female person living with disability, Nepal)
To support selected countries’ aspirations to reach 100% open defecation free (ODF) status, the SSH4A Results Programme focuses its attention on unserved groups by first, disaggregating data by age, gender, wealth, and other related inequalities. Second, by identifying who among them are “twice disadvantaged,” e.g., female elderly, poor and living in hard to reach areas, – so that we deploy more targeted sanitation interventions per household category.
Unpacking the ‘unserved’: SSH4A research methods
To effectively inform sanitation improvements in countries, SSH4A RP applies several tried and tested methods to make data explicit on diverse groups of people.
Regular monitoring. At the minimum, annual household (HH) surveys are conducted to measure sanitation progress from baseline to date. Some countries have established monitoring mechanisms conducted by communities, e.g., Tanzania. The surveys present data disaggregated by gender, disability, and wealth.
In Tanzania, SNV developed an innovative approach called Jirani Sanitation Groups (JSGs). 'Jirani' means neighbor, and the approach is based on community support; if a toilet collapses another can be built with the help of neighbours.
Jirani leaders monitor the progress of the 10 households closest to their homes, and sensitise their neighbours on the importance of building, taking care of, and improving sanitation and handwashing facilities. The leaders form committees that monitor sanitation and hygiene progress on the ground and report monthly to the village government.
Inclusive data collection is carried out by a programme staff with relevant stakeholders, e.g., government, community volunteers, etc. We work with a mixed representation of data collectors, including community members, to help identify and engage with households often left behind.
Participatory data review and analysis help us examine data against our plans, discern if our approaches yield results, and identify remedial actions. Our analysis examines how groups are faring, and how each can be supported better.
Policy influencing. In Kenya and Zambia for example, SSH4A RP participated in the revision of national data collection tools. Our inputs helped strengthen representation of people with disabilities. Today, both countries have baseline data, and regularly monitor incremental progress in people with disabilities’ access to latrines and handwashing facilities.
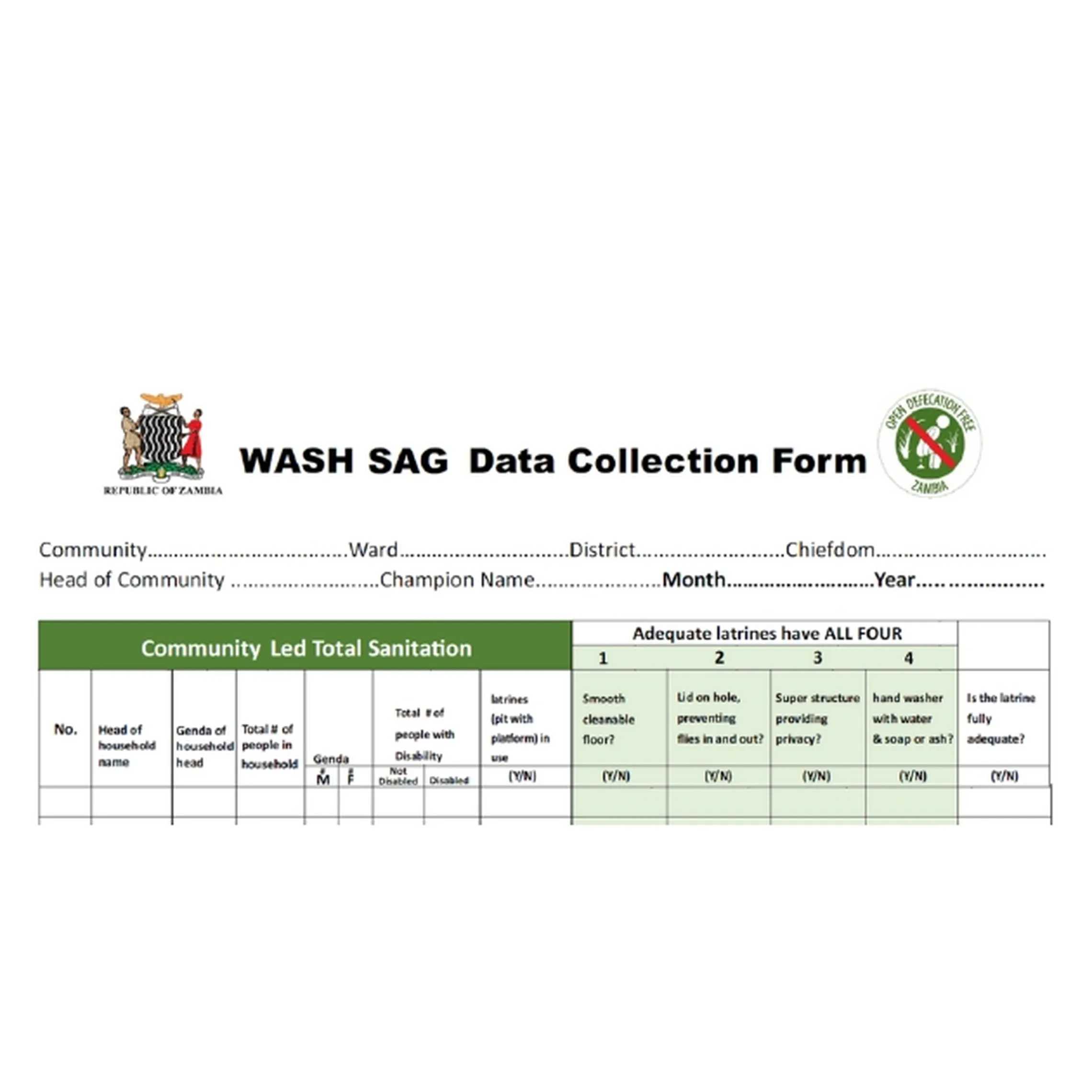
Sample Sanitation Action Group data sheet with info on gender and disability
Focus group discussions (FGDs). Although HH surveys yield relevant quantitative data, they hardly give explanatory insights. FGDs don’t only enrich our understanding of datasets, but they give unserved groups a voice. Through our FGDs, we realised that many women opt to not attend or speak in meetings facilitated by male health promoters. Hence, in countries such as Kenya, Tanzania and Nepal, we trained female health promoters to reach out to fellow women.
Collaboration with local leaders increases the legitimacy of the process, and enables households to speak up. Some households with members living with disabilities opt to remain silent for fear of further stigmatisation. In Ghana, on the other hand, working with traditional leaders uncovered several elderly persons living alone, with disabilities – some of whom were abandoned, or had chosen a life of isolation. During meetings, their relatives don’t mention them for fear of arrest due to elderly neglect.


Working with unserved groups: lessons
Over ten years of rural sanitation programming taught us that finding and eliciting the participation of unserved groups cannot be done using a single method. Simply using a singular method ascertains that someone will be left behind. We need mixed methods to be able to reach out to various groups.
Secondly, we need to recognise that individuals who have long been stigmatised may have internalised their exclusion from society. Overcoming this stigma takes time. We should provide a safe space for communities to engage with us on these issues.
Thirdly, many respondents complain of being asked too many questions by different stakeholders, yet nothing about their situation changes. We need to make sure that the process of data gathering is considered a learning process, rather than an extractive one. Communicating – with clarity – our interventions, and the type of support we can offer is necessary. For example, while community support can successfully bring households to basic levels of sanitation, such support can’t withstand climatic conditions.
Finally, in order to sustain progress and meet the SDGs, additional resources are needed to move groups from basic to safely managed levels of sanitation. The reality is... competing priorities at household level means that they can only invest in basic sanitation.
About the Author: Anne Mutta is multi-country programme manager of SNV’s largest Payment by Results (PbR) programme to date – a multi-million programme that is being implemented across eight countries in Africa and Nepal. Anne, based in Kenya, has 20 solid years of experience leading action-oriented and evidence-based WASH programmes.